
Here are some historical dates forever etched in memory:
July 4, 1776—American declaration of independence
December 7, 1941—Pearl Harbor
October 14, 1066—Battle of Hastings
August 3, 1492—Columbus sets sail
November 22, 1963—The assassination of John F. Kennedy
November 9, 1989—Fall of the Berlin Wall
September 11, 2001—9/11 terrorist attacks
For the families and caregivers of Alzheimer’s patients, June 7, 2021, and July 6, 2023, undoubtedly deserve a place on that list. These are the dates of the first two potentially disease modifying anti-Alzheimer drugs ever approved. The landmark approvals introduced ray of hope into this darkest and most desperate of situations despite some uncertainty over safety and effectiveness.
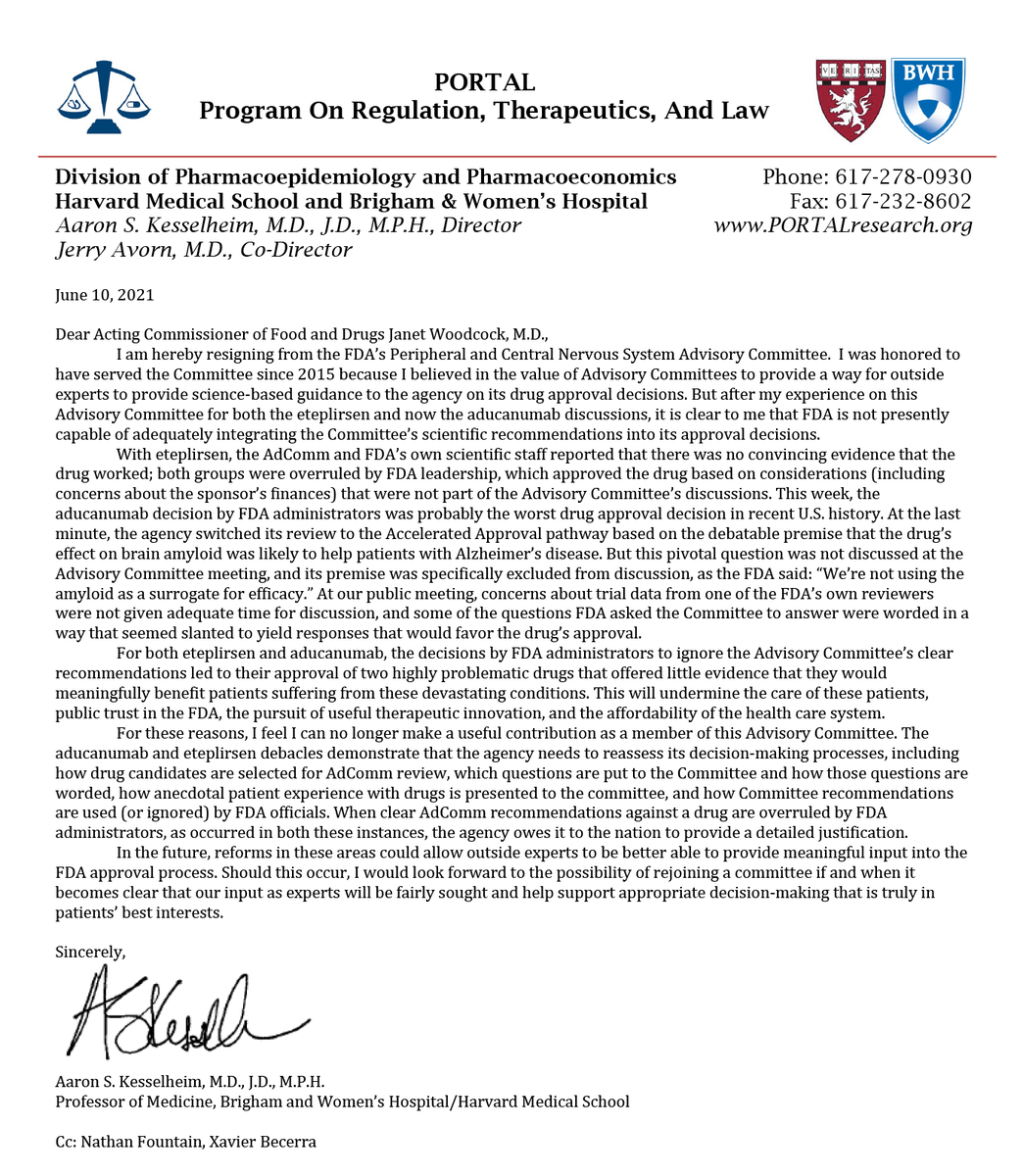
The first drug to be approved, controversially, against the backdrop of a near unanimous ‘no’ vote from the FDA’s Advisory Committee in 2021 was Biogen’s anti-amyloid monoclonal antibody (MAB), Aduhelm (aducanumab). Following the approval announcement, three members of the Advisory Committee publicly resigned in protest over what one member blasted as “a sham process”[1] and another as “probably the worst drug approval decision in recent U.S. history”.[2] The second drug to be approved somewhat less controversially in 2023 was Biogen’s and Eisai’s anti-amyloid MAB, Leqembi (lecanemab).
Downsides.
Responsible for the controversy are the several serious downsides and disadvantages of these MABs.
The first downside is the risk of life-threatening side effects such as swelling and bleeding in the brain, which led to 3 deaths during each of the Aduhelm and Leqembi trials. The second downside is the high intensity of treatment—Aduhelm is given by IV infusion for 45–60-minutes once a month and Leqembi is given by IV infusions for 45–60-minutes twice a month. The third is that both are indicated only for mild, early onset Alzheimer’s disease, which rules out approximately 80-85% of patients. The fourth is that Aduhelm did not noticeably improve patient outcomes and even though Leqembi slowed disease progression for 5.3 months compared to placebo, several neurologists, public health organizations, and patient advocates have gone on record to complain that this difference, even if statistically significant, is too slight to be clinically meaningful—in other words, these experts believe that the improvement is not enough for patients, physicians, or family members to notice.[3],[4],[5]
The real kicker, though, is the price—Aduhelm costs $28,200 per year and Leqembi costs $26,500 per year. These costs do not factor in the need for additional MRIs or PET scans and clinical visits to monitor for brain swelling or bleeding, which amounts to around $7,300, and patient out of pocket expenses that can easily reach into the several thousands of dollars despite Medicare coverage of Aduhelm and Leqembi.
Alzheimer’s disease (AD).
AD is a progressive, age-dependent neurodegenerative disorder, originally described in 1906 by the German psychiatrist and neuropathologist Aloysius “Alois” Alzheimer whose last name is inextricably linked to it. The disease gradually sets in with the loss of recent memory and thinking skills, sleep fragmentation, and behavioral and personality changes that collectively are severe enough to significantly interfere with independent daily activities.
The structural alterations of the brain in AD involve the build-up of amyloid beta (Aβ) plaques and tau protein tangles that accompany the onset of dementia. This term, dementia, encompasses a severe loss of brain function. Besides AD, which accounts for 60-80% of cases, other less common causes of dementia are cerebrovascular disease, Lewy body disease, Parkinson’s disease (PD), hippocampal sclerosis, frontotemporal lobar degeneration, and “mixed pathologies”.
Don’t forget about neuroinflammation.
The equivocal clinical significance of the Aduhelm and Leqembi clinical trials coupled with allegations of falsified Aβ research data from a seminal 2006 research publication seriously calls into question whether Aβ is indeed the long-sought-after smoking gun of AD, or just a red herring.
Gradually gaining momentum as the real root cause of AD and other neurodegenerative diseases is neuroinflammation. Regardless of the actual underlying factors, whether they are genetic, metabolic, dietary, environmental etc., all roads may lead, in fact, to neuroinflammation, in other words, inflammation in the central nervous system (CNS). If this is indeed the case, and more clinical research is needed to confirm, then the future of AD treatment may belong not to anti-amyloid MABs, but to therapies like EpicentRx’s nibrozetone (RRx-001) that directly inhibit the NLRP3 inflammasome, a protein structure that regulates the inflammatory response. Experimental data indicates that nibrozetone reduces AD-associated pathology and cognitive impairment.[6]
If the data continue to look good, one might reasonably expect to see nibrozetone enter clinical trials by 2025 as a treatment candidate for AD.
Save the date.
[1] https://www.washingtonpost.com/health/2021/06/09/alzheimers-drug-controversy/
[2] Letter from Dr. Aaron Kesselheim, Brigham and Women’s Hospital/Harvard Medical School, to Acting
Commissioner Janet Woodcock, M.D., Food and Drug Administration (June 10, 2021) (online at
https://pbs.twimg.com/media/E3jKN4GWYAUGj9U.png)
{kind=link}
[3] https://www.fiercehealthcare.com/payers/leqembi-approval-could-burden-medicare-system-critics-warn
[4] https://pink.pharmaintelligence.informa.com/PS147551/Eisais-Lecanemab-US-FDA-Showed-Flexibility-On-Clinical-Endpoint-Results-Safety-Database-Size
[5] Science. Scientists tie third clinical trial death to experimental Alzheimer’s drug. December 21, 2022. https://www.science.org/content/article/scientists-tie-third-clinical-trial-death-experimental-alzheimer-s-drug. Accessed January 4, 2023.
[6] https://alz-journals.onlinelibrary.wiley.com/doi/10.1002/alz.061516